The Iliotibial band or tract (ITB) is the bane of a runner’s existence and often the innocent victim of being the cause of knee pain.
By: Rebekah Hobbs
The Iliotibial band or tract (ITB) is the bane of a runner’s existence and often the innocent victim of being the cause of knee pain. However, there are lots of misconceptions around this truly remarkable piece of our anatomy. One of the misconceptions is that the ITB itself is the cause of the problem. This is not true as the ITB is not a contractile structure like a muscle. Rather, the ITB is comparable to a seat belt in its structure and tensile properties. It functions as both a lever for knee actions but mostly as a strut or support for both the hip and knee, kind of like a guy-rope of a tent.
Anatomy
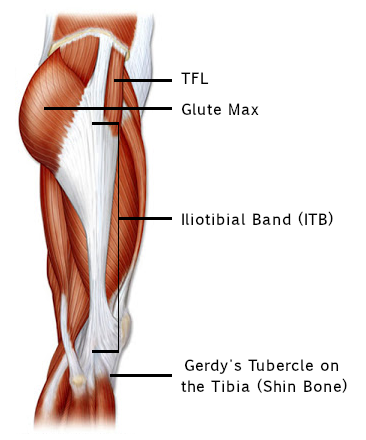
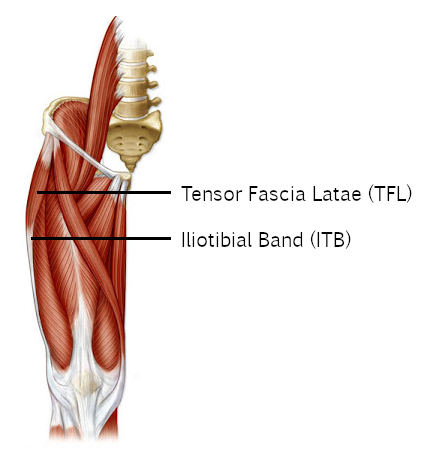
The anatomy of the ITB is interesting as it is made of connective tissue and resembles a blend of a tendon and a band of fascia. It starts from the musculotendinous junction of the Tensor Fascia Latae (TFL) muscle and extends down the side of the thigh and attaches to a projection on the side of Tibia (shin bone) called Gerdy’s Tubercle. The TFL starts on the front of the outside of the Ilium in the Pelvis/Hip region and extend to the ITB. The TFL performs abduction and flexion at the hip, tilts the pelvis anteriorly (forwards) and internally rotates a flexed hip.
Along, with the TFL the Gluteus Maximus (Glute Max) acts on the ITB to support and perform actions at the knee and hip. The Glute Max is the largest of the gluteal muscles; it starts on the back of the outside of the Ilium, sacrum, coccyx and lumbar fascia and runs to the Greater Trochanter of the femur and the ITB. The Glute Max performs the movements of extension and external rotation of the hip, as well as tilting the pelvis posteriorly (backwards). Because the Glute Max is a large muscle the fibres divide into two sections and travel at slightly different angle, this creates a 2-in-1 effect in the muscle. The upper fibres perform abduction of the hip/leg and the lower fibres perform adduction of the hip/leg.
Shortening or tightening of the TFL or Glute Max will cause the ITB to tighten as well, this causes postural changes to occur. If the TFL is causing the tightening of the ITB, it then pulls the pelvis into an anterior (forward tilt). An anterior tilt of the pelvis causes an increased lordosis or curve in the low back. If the Glute Max is causing the ITB to tighten, then the pelvis is pulled into a posterior (backwards) tilt. A posterior pelvic tilt causes a flat low back or slouching posture. Both of these incorrect postures can cause low back pain and other postural problems.

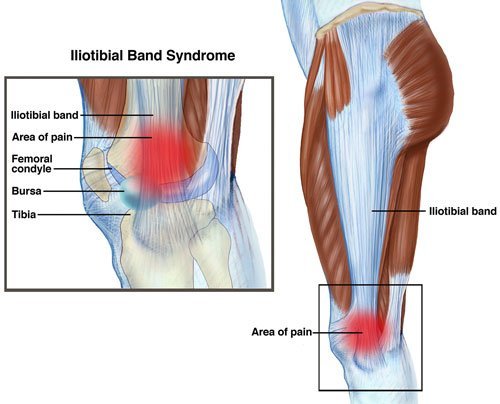
Iliotibial Band Friction Syndrome
ITB Friction Syndrome (ITBFS) is a painful condition felt at the knee. It is often described by a burning, aching or tenderness on the outside of the knee and can be accompanied by a snapping or popping sound. The pain usually occurs on bending or straightening the knee. ITBFS is usually caused by a biomechanical dysfunction at either the bones or muscles.
ITFS is caused when the ITB is pulled too tight by muscular imbalances of the TFL and Glute Max or bony deformity, usually at the knee. The taught ITB then creates increased friction as it moves over the lateral femoral condyle (bony protrusion on femur above the knee) during bending and straightening of the knee. A naturally occurring bursa is present to prevent injury to the ITB from a normal friction load, however as the load increases the bursa is unable to perform its function and becomes inflamed. The inflammation of the bursa and tendon is what causes the pain and can also cause redness and swelling when severe. The snapping or popping sound that can occur is caused by the taught ITB flicking over the lateral femoral condyle, kind of like when flicking a guitar string.
Common causes of ITBFS are:
- Bow Legs
- Osteoarthritis of the Knee
- Leg Length Discrepancy
- Muscle weakness in the abdominal canister, gluteals and the hip
Sports and activities that involve repetitive flexion and extension of the knee are prone to causing ITBFS. These sports include: running, cycling, hiking, long distance walking and other activities like cross fit. ITBFS is easily treatable and preventable without surgical intervention.
Tips to prevent ITBFS include:
- A good warm up, cool down and stretching regime
- Incorporating sufficient recovering time into your weekly exercise regime
- Wearing the correct shoes for your feet
- Running on a flat surface or alternating the side of the road you run on. Most roads have a camber or tilt so one leg will always work harder than the other causing muscle imbalances.
- Foam rolling for endurance sports such as long distance running, cycling and triathlons is an important part of a recovery regime
- Get a running analysis
- Get a biomechanical analysis
ITB’s are wonderful support structures that literally strut the hip and knee, while you strut your stuff be it in the mall or on the run. It’s important to remember that problems at the ITB are only the indication of a problem elsewhere that needs to be addressed. If you are concerned that you might have ITBFS or are participating in a high level sport that involves repetitive motions at the knee, please contact your physiotherapist for treatment and assessment.
Prevention is always better than cure and the quicker you deal with the problem the quicker you can be back to confidently strutting your stuff pain-free!